From Specific to Universal Stanford’s Immune Reboot
For more than two centuries, vaccines have followed a remarkably consistent principle. Expose the immune system to a weakened or partial version of a pathogen and allow it to develop memory. When the real infection arrives, the body responds faster and more effectively. From smallpox to polio to measles, this strategy has saved hundreds of millions of lives. Yet it has one important limitation. Each vaccine is designed for a specific pathogen. When viruses mutate or when new microbes emerge, protection must be redesigned and redeployed.

Researchers at Stanford Medicine have now proposed something radically different. In a recent study published in the journal Science, a team led by Professor Bali Pulendran describes what they call a universal vaccine formula delivered as a nasal spray. Instead of targeting a single virus or bacterium, this approach appears to provide broad protection in mice against a wide array of respiratory viruses, certain bacteria, and even allergens. If these findings translate into humans, the implications could reshape public health strategies, pandemic preparedness, and seasonal infection control.
Traditional vaccines primarily train the adaptive immune system. Adaptive immunity involves highly specific responses carried out by B cells and T cells that recognize distinct molecular signatures called antigens. This specificity is powerful but narrow. Influenza viruses mutate frequently, which is why flu shots are reformulated annually. The rapid emergence of SARS CoV 2 variants during the COVID 19 pandemic also demonstrated how viral evolution can challenge vaccine effectiveness.
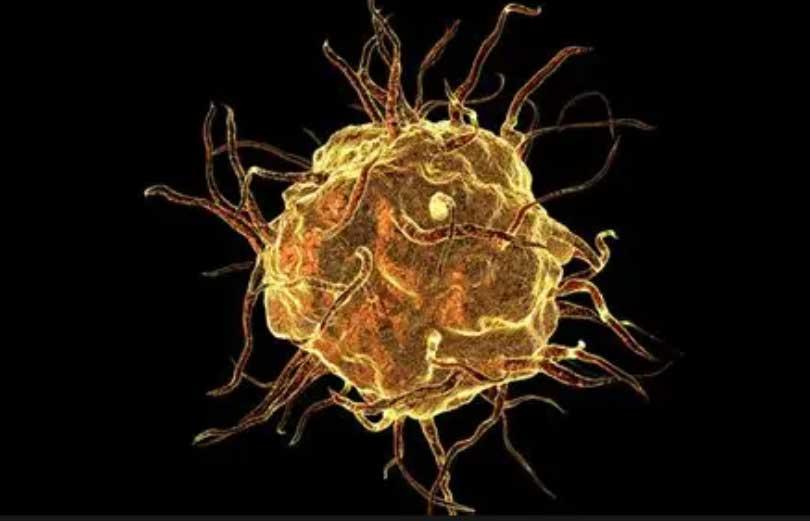
The Stanford approach departs from this model. Rather than focusing on adaptive immune memory against one target, the nasal formulation appears to enhance the innate immune system, particularly immune cells known as macrophages in the lungs. The innate immune system is the body’s first line of defense. It responds quickly but has historically been considered nonspecific and lacking memory. However, emerging research over the past decade has shown that innate immune cells can undergo a form of functional reprogramming often referred to as trained immunity. After certain stimuli, these cells respond more robustly to later infections, even if those infections are unrelated to the original trigger.
In the Stanford study, mice received the formulation intranasally. The treatment appeared to reprogram lung macrophages into a heightened state of readiness. When exposed to respiratory viruses, treated animals showed dramatic reductions in viral load compared with untreated controls. According to the researchers, viral replication in the lungs was reduced by 100 to 1000-fold in some experiments. The protective effect lasted for approximately three months in mice.
In addition to viral protection, the treatment also reduced susceptibility to bacterial pathogens including Staphylococcus aureus and Acinetobacter baumannii, both of which can cause serious respiratory infections.
Perhaps most intriguingly, the nasal spray also appeared to modulate allergic responses. In mouse models exposed to house dust mite allergens, animals that received the formulation demonstrated reduced inflammatory responses associated with allergic asthma. This suggests that the immune recalibration induced by the spray may not only enhance defense against pathogens but also rebalance inappropriate inflammatory reactions.

The idea of broad immune activation is not entirely unprecedented. The Bacillus Calmette Guérin vaccine, originally developed against tuberculosis, has long been observed to confer nonspecific protective effects against other infections. Studies have suggested that BCG vaccination may reduce all-cause mortality in certain populations, potentially through mechanisms involving trained innate immunity. The Stanford research builds upon this conceptual framework but applies it locally to the lungs, the primary site of respiratory infection.
The lungs represent a critical battleground in infectious disease. Many respiratory pathogens gain entry through inhalation and establish infection in the airway mucosa before spreading systemically. By priming immune cells directly at this entry point, the nasal spray strategy aims to intercept pathogens at the earliest stage. This localized immune readiness may prevent viruses from establishing high levels of replication, thereby reducing disease severity and possibly transmission.
The potential public health applications are significant. Each winter, communities face a convergence of respiratory threats including influenza, respiratory syncytial virus, seasonal coronaviruses, and various bacterial pneumonias. Vaccination campaigns often require separate formulations for each pathogen and rely on high levels of public uptake. A single seasonal nasal spray that enhances broad lung immunity could simplify logistics and increase accessibility, especially for individuals who avoid injections.
In the context of emerging pandemics, such a tool could provide an important bridge. During the early months of the COVID-19 pandemic, no vaccines were available. A broad acting immune enhancer could theoretically reduce disease severity and mortality while pathogen specific vaccines are being developed and distributed. Professor Pulendran has suggested that this approach would complement rather than replace conventional vaccines, particularly in the early stages of an outbreak.
Despite the promise, substantial questions remain. The findings to date are based on animal studies. Mouse immune systems differ in important ways from those of humans. Laboratory mice are often immunologically naive and live in controlled environments.
Human immune systems, by contrast, are shaped by decades of infections, vaccinations, environmental exposures, and microbiome interactions. Whether a similar degree of immune reprogramming can be achieved safely in people is unknown.
Duration of protection is another key issue. In mice, the effect lasted around three months. It is unclear whether repeated dosing would maintain effectiveness or whether the immune system might adapt in ways that reduce responsiveness over time. Persistent immune activation also raises safety concerns. An immune system that is chronically dialed up could increase the risk of inflammatory disorders or autoimmune reactions. External experts have cautioned about the possibility of what some describe as friendly fire, in which an overactive immune system damages healthy tissue.
Delivery mechanisms may also require refinement. While a nasal spray is effective in small animals, ensuring adequate distribution to the lower airways in humans may require nebulized administration. Clinical trials will need to determine optimal dosing, delivery methods, and safety profiles.
The researchers plan to conduct human studies, potentially including controlled human infection models under strict ethical oversight. Such trials could provide early insights into whether the formulation reduces viral load, shortens illness duration, or alters inflammatory markers in people. Only through carefully designed clinical research can the balance between benefit and risk be established.
The broader scientific context is important. Immunology has evolved significantly in recent years, particularly in understanding the plasticity of innate immune responses. Epigenetic changes, metabolic reprogramming, and altered cytokine signaling pathways have all been implicated in trained immunity. If the Stanford formulation successfully harnesses these mechanisms in a controlled and temporary manner, it could represent a new class of immunomodulatory intervention rather than a conventional vaccine.
There are also global equity implications. Needle free administration could facilitate mass distribution in low resource settings. Reduced dependence on cold chain logistics and simplified seasonal campaigns could improve coverage rates. At the same time, affordability, manufacturing scalability, and regulatory pathways will determine whether such a product becomes widely accessible.
The excitement surrounding this research is tempered by the recognition that many promising animal studies do not ultimately translate into clinical success. The history of biomedical innovation includes numerous examples of therapies that appeared transformative in preclinical models but proved less effective or less safe in humans. Rigorous peer review, replication, and phased clinical trials will be essential.
Even if the universal nasal vaccine does not fully replace pathogen specific vaccines, it may still find a valuable niche. It could serve as an adjunctive therapy for high-risk populations during peak respiratory seasons. It could provide temporary protection for frontline healthcare workers during outbreaks. It might even offer new therapeutic strategies for allergic and inflammatory lung diseases.
At its core, the Stanford research challenges a deeply ingrained paradigm. Since the late eighteenth century, when Edward Jenner pioneered vaccination against smallpox, the field has largely focused on specificity. The idea that immune protection can be broad, flexible, and locally enhanced represents a conceptual shift. Instead of teaching the immune system to recognize a single enemy, the new strategy seeks to heighten general vigilance at the point of entry.
Whether this approach will ultimately transform medical practice remains uncertain. The path from laboratory discovery to approved human therapy is long and complex. Yet the study underscores a growing recognition that immunity is more adaptable than once believed. By exploring new ways to harness innate immune mechanisms, scientists may expand the toolbox for preventing infectious disease in an increasingly interconnected world.
If human trials confirm safety and efficacy, a seasonal nasal spray that strengthens lung defenses against multiple pathogens could become a powerful addition to modern medicine. It would not eliminate the need for targeted vaccines, but it might provide a versatile shield during periods of heightened respiratory risk. For now, the universal vaccine remains a compelling scientific possibility grounded in promising animal data and awaiting the decisive test of human evidence.
Sources:
- Pulendran B et al., Science (2024).
- Netea MG et al., Science (2016).
- Stanford Medicine News Center (2024).
- Expert commentary from University of Oxford and Liverpool School of Tropical Medicine.
